Abstracts
INTRODUCTION: Chronic liver disease results in large functional impact, causing loss of muscle mass and function with consequent reduction of functional capacity. OBJECTIVE: To evaluate and compare the respiratory muscle strength and functional capacity of candidates for liver transplantation who are under Class B or C according to Child Pugh Score and to correlate these variables within each group. METHODS- Cross-sectional study with a convenience sample of 35 patients divided into two groups based on the score obtained in the Child Pugh Score B (19 patients) and Child Pugh Score C (16 patients). All subjects were evaluated in a single moment, and the maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP) as well as the distance walked during the 6-minute walk test (6MWT) were measured. RESULTS: Individuals classified with Child Pugh Score B showed higher values in the MIP (- 86.05 vs. 23.89 - 57.94 14.14), p = 0.001, in MEP (84.16 vs. 28.26 72.00 16 1994), p = 0.142, and the distance walked in 6MWT (473.63 vs 376.13 39.00 55.276), p = 0.001. We also found a positive correlation between the values of MIP and distance walked during 6MWT in group B of the Child Pugh Score, r = 0.64 and p = 0.003. CONCLUSION: The progress of liver disease contributes to the onset of several complications, which together appear to contribute to the reduction of functional capacity of individuals. In our study this was evidenced by the worse performance of Child Pugh score C group. This may suggest that the wait for liver transplantation (LTx) can worsen the functional capacity of these individuals.
liver disease; functional capacity; respiratory muscle strength; Child-Pugh score
INTRODUÇÃO: A doença hepática crônica resulta em grande impacto funcional, causando perda de massa e função muscular com consequente redução da capacidade funcional. OBJETIVO: Avaliar e comparar a força muscular respiratória e a capacidade funcional dos candidatos ao transplante hepático que possuem classe B ou C segundo o Child-Pugh Score e correlacionar estas variáveis dentro de cada grupo. MÉTODOS: Estudo transversal, com amostra de conveniência composta por 35 pacientes, divididos em dois grupos a partir da pontuação obtida no Child-Pugh Score, sendo B (19 pacientes) e C (16 pacientes). Todos os indivíduos foram avaliados em um único momento, sendo mensuradas as pressões inspiratória máxima (PImáx) e expiratória máxima (PEmáx) e a distância percorrida no teste de caminhada de seis minutos (TC6M). RESULTADOS: Os indivíduos classificados com Child-Pugh Score B apresentaram maiores valores na PImáx (-86,05 ± 23,89 vs. -57,94 ± 14,14), p = 0,001, na PEmáx (84,16 ± 28,26 vs. 72,00 ± 16,94), p = 0,142, e na distância percorrida no TC6M (473,63 ± 55,276 vs. 376,13 ± 39,00), p = 0,001. Encontramos, ainda, correlação positiva entre os valores da PImáx e a distância percorrida no TC6M dentro grupo Child-Pugh Score B, r = 0,64 e p = 0,003. CONCLUSÃO: O progresso da doença hepática contribui para o surgimento de diversas complicações que, em conjunto, parecem contribuir para a redução da capacidade funcional dos indivíduos. Em nosso trabalho, isso ficou evidenciado pelo pior desempenho do grupo Child-Pugh Score C. Isto pode sugerir que a espera para o transplante hepático (TxH) pode agravar a capacidade funcional e a força muscular respiratória desses indivíduos.
doença hepática; capacidade funcional; força muscular respiratória; escore Child-Pugh
ORIGINAL ARTICLE
EXERCISE AND SPORTS MEDICINE CLINIC
IMethodist University Center-IPA
IIFederal University of Health Sciences of Porto Alegre
IIIMethodist University |enter -IPA and Federal University of Rio Grande do Sul
IVFederal University of Rio Grande do Sul
Mailing address
ABSTRACT
INTRODUCTION: Chronic liver disease results in large functional impact, causing loss of muscle mass and function with consequent reduction of functional capacity.
OBJECTIVE: To evaluate and compare the respiratory muscle strength and functional capacity of candidates for liver transplantation who are under Class B or C according to Child Pugh Score and to correlate these variables within each group. Methods - Cross-sectional study with a convenience sample of 35 patients divided into two groups based on the score obtained in the Child Pugh Score B (19 patients) and Child Pugh Score C (16 patients). All subjects were evaluated in a single moment, and the maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP) as well as the distance walked during the 6-minute walk test (6MWT) were measured.
RESULTS: Individuals classified with Child Pugh Score B showed higher values in the MIP (- 86.05 vs. 23.89 - 57.94 14.14), p = 0.001, in MEP (84.16 vs. 28.26 72.00 16 1994), p = 0.142, and the distance walked in 6MWT (473.63 vs 376.13 39.00 55.276), p = 0.001. We also found a positive correlation between the values of MIP and distance walked during 6MWT in group B of the Child Pugh Score, r = 0.64 and p = 0.003.
CONCLUSION: The progress of liver disease contributes to the onset of several complications, which together appear to contribute to the reduction of functional capacity of individuals. In our study this was evidenced by the worse performance of Child Pugh score C group. This may suggest that the wait for liver transplantation (LTx) can worsen the functional capacity of these individuals.
Keywords: liver disease, functional capacity, respiratory muscle strength, Child-Pugh score.
INTRODUCTION
Hepatic cirrhosis is characterized by the diffuse substitution of the normal hepatic structure for nodules of abnormal structure surrounded by fibrosis and is present in the final stage of a series of pathological processes derived from many causes(1). Hepatic disease causes great nutritional impact, regardless of its etiology, since the liver performs many biochemical reactions, such as production, alteration and use of nutrients and substances metabolically important to the body (2-4).
One of the complications caused by developed hepatic disease are the metabolic alterations associated with the patients' malnutrition, since they lose great quantity of muscular mass, presenting hence, alterations in functionality, which provides a physical inactivity scenario. The association of all these factors causes negative influence in the activities of daily living (ADL) and in the quality of life of this population(5-7). In a previous study carried out by our group, alterations in the frequency and severity of hepatic diseases, as well as in the functionality and quality of life of the individuals with severe hepatic disease and who are on the waiting list for an hepatic transplant was found (LTx)(8).
Due to the increase in the number of candidates to LTx, classification models with several clinical variables were created to determine the severity of the hepatic disease. Initially, the Child-Pugh Score was created and recently the Model for End Stage Liver Disease (MELD) has also been used in the daily practice. The former was traditionally used in the stratification of pre-surgical risks and the latter was especially used to prevent survival three months after transplant, using for its classification, serum values of bilirubin and creatinine, and coagulation proof. The MELD punctuation ranges from 0 to 40, where it is inversely proportional to the score and survival ratio(9-11). The Child-Pugh Score uses variables such as bilirubin and serum albumin, prothrombin time and presence of ascites and encephalopathy. The higher the punctuation the worse the clinical status of the individual and the clinical "decompensation" status which indicates hepatic cirrhosis should be higher or equal to 7 (class B). This class is a criterion accepted for inclusion of the patients on the waiting list for the LTx(12).
Early indication to LTx made it possible to patients to reach survival rate above 70% in five years, and also reduced the treatment costs. Moreover, it is important to highlight that the patients who use medication treatment for the disease at final stage present mortality of 70% per year(13,14). These data caused that the search for the surgical procedure for the hepatic disease solution significantly increased. Thus, many candidates spend a long period on the waiting list, which favors the onset of new complications which, on their turn, worsen the functionality of these individuals.
However, none of the models devised to grade the hepatic disease stage uses functional variables. The performance of the six-minute walking test (6MWT) is an efficient measurement of the exercise submaximal capacity which presents strong correlation with the functional capacity(15). It has been demonstrated that individuals who complete a shorter distance in the test present increase in mortality derived from the advanced hepatic disease(16).
It is also believed that due to the presence of ascites (50% to 60% of the cases), a mechanical disadvantage in the diaphragm muscle occurs, which may possibly interfere in the length-tension of the muscle and, consequently, in the respiratory muscular strength, harming even more the functionality of the individuals(17).
Although there is great variety of studies approaching the hepatic disease and its stages, little is seen on the functional capacity of this population. We believe that the understanding on the limitations of these individuals may contribute to a more accurate approach, which enables to reach a better recovery post-LTx, reintegrating them more rapidly to their new ADL.
This study has the aim to evaluate and compare the respiratory muscle strength and functional capacity of patients candidates to LTx who are under class B or C according to the Child-Pugh Score and, subsequently, to correlate these variables within each group.
MATERIALS AND METHODS
This study was transversal and 35 adult patients who were under supervision in the Hepatic Transplant Service of the Santa Casa Hospital Complex of Porto Alegre between February and November,2009 have been recruited. All individuals who presented clinical conditions to perform all the proposed procedures as well as those who were on the waiting list for the hepatic transplant were included in the study. Exclusion criteria were the presence of severe encephalopathy (level III and IV), severe degenerative diseases, such as muscular dystrophy and multiple sclerosis, hemodynamic instability or any other factor which hampered the performance of the proposed procedures. No exclusion occurred during the study. The patients were selected after verification of their medical records. The Child-Pugh Score variables provided minimum punctuation of 1 and maximum of 3 and the final punctuation ranged between 5 and 15. Subsequently, the individuals were classified in A (from 5 to 6 points), B (from 7 to 9 points), or C (above 10 points). The entire procedure was performed by the clinical staff of the hospital. The medical records verification was performed in the maximum time of 15 days before the functional evaluation so that no difference between the medical and physiotherapeutic follow-up would occur.
The patients performed in a single moment the following evaluation: data and samples' characteristics recording through an assessment slip specifically devised, evaluation of the respiratory muscles strength through manovacuometry and the 6MWT. The measurements were always performed by the same evaluator.
The Free and Clarified Consent Form of each patient was obtained and the work was approved by the Ethics and Research Committees of the Methodist University Center at IPA and the Santa Casa Hospital Complex of Porto Alegre.
In order to measure the strength of the respiratory muscles, a digital manovacuometer MVD 500 brand name Globalmed®, which was always calibrated before each data collection was used. MIP was evaluated with the individual performing maximal expiration, until the residual volume (RV), and, after suitable positioning of the equipment in the patient's mouth, maximal forced inspiration was performed. In order to have the MEPobtained, the individual was asked to begin the maneuver from the total pulmonary capacity, which was followed by a maximal forced expiration. The maneuvers were performed with the equipment being suitably positioned in the patient's mouth so that no flaw would occur in the test. A nasal clip was used to avoid air escape and there was the drain hole in the manovacuometer. The maneuver needed to be sustained for at least one second, and a total time of it of at least two seconds, in which the peak pressure was verified. The results were obtained after performance of five maneuvers, with minimum interval of one minute between them, and at least three acceptable maneuvers were obtained; that is to say, the values did not vary from each other more than 10%. The highest pressure in water centimeters was recorded (cmH2O), and the normality values supported by the Brazilian Pneumology and Tisiology Society were used(18,19).
The 6MWT was performed on a straight, flat, 30-meter long corridor, with not any kind of obstacle. Prior to the test beginning, all patients received instructions from the evaluator and during it standardized verbal stimuli were given at every walking minute, when the patients were encouraged to complete the longest distance possible. At the end of the test, the completed distance was measured. The patients were monitored through the respiratory rate, heart rate and oxygen peripheral saturation, using a Nonin oxymeter (9500, USA), and dyspnea sensation and fatigue in lower limbs were measured through the modified Borg's scale (0-10 scale), according to the American Thoracic Society (ATS)(15). All variables previously described were measured before and after the walking test, except for the distance, which was only quantified after the 6MWT.
STATISTICAL ANALYSIS
Statistical analysis was performed in the SPSS program (Statistical Package for Social Sciences) version 16.0. Data normality was verified with the Kolmogorov-Smirnov test. Student's t test was used for the comparisons of the means of the muscle strength variables (MIPand MEP), distance completed in the 6MWT, anthropometric and clinical characteristics between the two groups, and for the correlations between variables, the Pearson correlation test was used. Significance level adopted was p < 0.05.
RESULTS
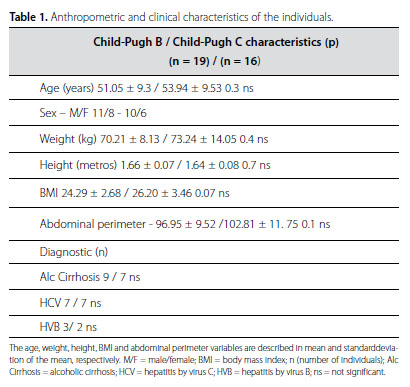
In our study, 35 patients have been evaluated and no loss or exclusion has occurred. The sample's anthropometric characteristics are described in table 1. Nineteen individuals were classified as Child-Pugh Score B and 16 as Child-Pugh Score C. Alcoholic cirrhosis diagnosis was found in nine patients from group B and in seven from group C; viral hepatitis by virus C (HVC) in seven patients from both groups; and viral hepatitis by virus B (HVB) in three patients from group B and in two from group C. The time of the disease diagnosis is not significantly different from groups B and C, 14 ± 3 vs. 12 ± 5 months, respectively (p = 0.9). There was not significant difference between groups concerning the clinical and anthropometric variables. Concerning the drug therapy in both groups, they were similar, since the use of antiretroviral medication in patients with the viral processes is usually equivalent.
Table 2 presents the comparison of the 6MWT variables of the two assessed groups. No difference has been found between the two groups in the values which preceded the test and the values after it.
The Child-Pugh Score B group presented higher values in the MIP (cmH2O), -86.05 ± 23.89 vs. -57.94 ± 14.14, p = 0.001 in the MEP (cmH2O), 84.16 ± 28.26 vs. 72.00 ± 16.94, p = 0.142, and in the distance completed in the 6MWT (meters), 73.63 ± 55.276 vs. 376.13 ± 39.00, p = 0.001 (Table 3).
Positive correlation was also found between the MIP values and the distance completed in the 6MWT within the Child-Pugh Score B group, r = 0.64 and p = 0.003 (Figure1), a fact which was not verified in the Child-Pugh Score C group.
DISCUSSION
The individuals with hepatic disease develop a malnutrition scenario due to decrease in food intake, deficit in absorption and transport of nutrients and increase of the energetic cost at rest(20,21). In our study, the patients of both groups presented mean body mass index (BMI) which does not correspond to a malnutrition and cachexia episode.
The patients of this study, classified as Child-Pugh Score C, presented shorter completed distance in the 6MWT and lower values in the respiratory muscle strength than those classified as Child-Pugh Score B. In the study performed by Leitão et al.(22), it was observed that the individuals who wait for an hepatic transplant complete mean of 383.8 meters in the 6MWT, which corroborates our findings here. Alameri et al.(16) also evaluated the functional capacity of the patients candidate to hepatic transplant through the 6MWT, and the mean completed distance was 306 meters of the Child-Pugh Score C patients, and these patients presented also the worst performance and survival rate when compared to the individuals classified as B and A.
The 6MWT presents good correlation with the oxygen maximal consumption ( O2)(23). Dharancy et al.(24) demonstrated that majority of the cirrhotic patients presents lower peak O2 values than the expectation. Moreover, Epstein et al. verified that class A patients from the Child-Pugh Score presented better peak O2 values when compared to the individuals from the groups B and C(25).
O2)(23). Dharancy et al.(24) demonstrated that majority of the cirrhotic patients presents lower peak O2 values than the expectation. Moreover, Epstein et al. verified that class A patients from the Child-Pugh Score presented better peak O2 values when compared to the individuals from the groups B and C(25).
Another factor which contributes to the harm in the functional capacity of this population are the abnormalities in the gas exchanges. The most relevant of these abnormalities is unsuitable oxygenation of the arterial blood, since the difference in the oxygen alveolus-arterial ratio (P[A-a]O2) is increased in about 50% of the cases. Przybylowski et al.(26) investigated 104 patients and demonstrated that the individuals who had hepatic disease presented lower partial pressure of arterial oxygen (PaO2), lower capacity of carbon monoxide diffusion (DLco) and greater difference on the oxygen alveolus-arterial ratio (P[A-a]O2) when compared to the group which did not present cirrhosis. The investigators also found positive correlation between P(A-a)O2 and the Child-Pugh Score and negative correlation between DLco and the Child-Pugh Score.
Regarding the respiratory musculature strength, there are few findings in the literature. Carvalho et al.(17) verified that those individuals with higher mortality on the waiting list to undergo an hepatic transplant presented lower values of MIP than those in the control group. Our findings suggest that the Child-Pugh Score C group presents reduction in MIP when compared to the Child- Pugh Score B group, demonstrating that the hepatic disease progression compromises the respiratory musculature as well, either by the mass loss or by interference in the length-tension of the muscle.
When the MIP values were correlated with the completed distance in the 6MWT statistical significance was only obtained in the Child-Pugh Score B group. The complications already mentioned seem to have contributed so that the individuals classified as Child-Pugh Score C did not present correlation between variables; compromising factors, such as ascites and hepatic encephalopathy, may have disturbed their assessment.
Our study presents some limitations, especially with the control of nutritional variables. The BMI analysis may not reflect the actual nutritional aspect of the sample due to the presence of ascites in some patients. Medication administration may be a confusing variable, since at the exacerbation moment of the hepatic disease other pharmacological resources, such as corticosteroids, which negatively interfere on the musculoskeletal system, can be used. Another limitation refers to the sample size existing in both groups.
CONCLUSION
The hepatic disease progression contributes to the onset of many complications which as a set tend to reduce the functional capacity of this population. Such fact has been evidenced in our study through worse performance of the Child-Pugh Score C group, which presents a severe clinical status, suggesting hence that the wait for an hepatic transplant (LTx) may aggravate the functional capacity and respiratory muscle strength of these individuals.
REFERENCES
- 1. Lida VH, da Silva TJA, da Silva ASF, da Silva LFF, Alves VAF. Cirrose hepática: Aspectos morfológicos relacionados às suas possíveis complicações. Um estudo baseado em necrópsias. J Bras Patol Med Lab 2005;41:29-36.
- 2. Maio R, Dichi JB, Burini SC. Consequências nutricionais das alterações metabólicas dos macronutrientes na doença hepática crônica. Arq Gastroenterol 2000;37:52-7.
- 3. Sarin SK, Dhingra N, Bansal A, Malhotra S, Guptan RC. Dietary and nutritional abnormalities in alcoholic liver disease: a comparison with chronic alcoholics without liver disease. Am J Gastroenterol 1997;92:777-83.
- 4. Nompleggi DJ, Bonkovsky HL. Nutritional supplementation in chronic liver disease: an analytical review. Hepatology 1994;19:518-33.
- 5. Younossi ZM, Guyatt. Quality-of-Life Assessments and Chronic Liver Disease. Am J Gastroenterol 2006;93:1037-41.
- 6. Younossi ZM. Chronic liver disease and health-related quality of life. Gastroenterology 2001;120:305-7.
- 7. Gutteling JJ, de Man RA, Kiwi M, Boparai N, King D. Determinants of quality of life in chronic liver patients. Aliment Pharmacol Ther 2006;23:1629-35.
- 8. Barcelos S, Dias AS, Forgiarini Jr LA, Monteiro MB. Transplante Hepático: repercussões na capacidade pulmonar, condição funcional e qualidade de vida. Arq Gastroenterol 2008;45:186-90.
- 9. Hoteit AM, Ghazale AH, Bain JA, Rosenberg ES, Easley KA, Anania FA, Rutherford RE. Model for end stage liver disease versus Child Score in predicting the outcome of surgical procedures in patients with cirrhosis. World J Gastroenterol 2008;14:1774-80.
- 10. Child CG II, Turcotte JG. Surgery and portal hypertension. In: Child CG III, ed. The Liver and Portal Hypertension. Philadelphia, PA: Saunders; 1964:50-8.
- 11. Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P, Kremers W, Lake J, Howard T, Merion RM, Wolfe RA, Krom R. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 2003;124:91-6.
- 12. Carrithers RL Jr. Liver transplantation. American Association for the Study of Liver Diseases. Liver Transpl 2000;6:122-35
- 13. Devlin J, O'Grady JG. Indications for and Assessment in Adult Liver Transplantation: a Clinical Guideline. British Med Jour 1999;45:11-22.
- 14. Lucey MR, Brown KA, Everson GT, Fung JJ, Gish R, Keefe EB, et al. Minimal criteria for placement of adults on the liver transplant waiting list: report of national conference organized by the American Society of Transplant Physicians and the American Association for the Study of Liver Disease. Transplantation 1998;66:956-62.
- 15. Brooks D, Solway S, Gibbons WJ. ATS Statement on six minute walk test. Am J Resp Crit Care Med 2003;167:1287.
- 16. Alameri HF, Sanai FM, Al Dukhayil M, Azzam NA, Al-Swat KA, Hersi AS, Abdo AA. Six minute walk test to asses functional capacity in chronic liver disease patients. World J Gastroenterol 2007;13:3996-4001.
- 17. Carvalho EM, Iserm MRM, Lima PA, Machado CS, Biaagini AP, Massarollo PCB. Força muscular e mortalidade na lista de espera de transplante de fígado. Rev Bras Fisioter 2008;12:235-40.
- 18. Sociedade Brasileira de Pneumologia e Tisiologia. Diretrizes para Testes de Função Pulmonar. J Pneumol 2002;28:1-221.
- 19. Black LF, Hyatt RE. Maximal respiratory pressures: normal values and relationship to age and sex. Am Rev Resp Dis 1969;99:696-702.
- 20. Maio R. Indicadores nutricionais e gravidade da disfunção hepatocelular. Rev Bras Nutr Clin 1999;14:93-4.
- 21. Prijatmoko D, Strauss BJG, Lambert JR, Sievert W, Stroud DB, Wahlqvist ML, et al. Early detection of protein depletion in alcoholic cirrhosis: role of body composition analysis. Gastroenterology 1993;105:1839-45.
- 22. Leitão AV, Castro CL, Basile TM, Souza TH, Braulio VB. Avaliação da capacidade física e do estado nutricional em candidatos ao transplante hepático. Rev Assoc Med Bras 2003;49:424-8.
- 23. Miyamoto S, Nagaya N, Satoh T, Kyotani S, Sakamaki F, Fujita M, et al. Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension: comparison with cardiopulmonary exercise testing. Am J Respir Crit Care Med 2000;161:487-92.
- 24. Dharancy S, Lenyze M, Boleslawsky E, Neviere R, Declerck N, Canva V, Wallaert B, Mathurin P, Pruvot FR. Impact of impaired aerobic capacity on liver transplant candidates. Transplantation 2008;86:1077-83.
- 25. Epstein SK, Ciubotaru RL, Zilberberg MD, Kaplan LM, Jacoby C, Freeman R, et al. Analysis of impaired exercise capacity in patients with cirrhosis. Dig Dis Sci 1998;43:1701-7.
- 26. Przybylowski T, Krenke R, Fangrat A, Nasilowski J, Grabczak EM, Styczynski G, et al. Gas exchange abnormalities in patients listed for liver transplantation. J Physiol Pharmacol 2006;57:313-23.
Functional capacity and respiratory muscle strength of candidates to hepatic transplant
Publication Dates
-
Publication in this collection
20 Jan 2012 -
Date of issue
Oct 2011