Abstract
INTRODUCTION: Anemia is a nutritional problem of global importance. It is estimated that at least one-third of the population has been at one time anemic. OBJECTIVE: To evaluate the prevalence of anemia and associated factors in patients of a children's hospital in Recife. METHODS: A cross-sectional study was developed involving 595 male and female children aged from 6 to 59 months old, who were hospitalized in 2007. RESULTS: Children with a hemoglobin concentration less than 11 g/dL were considered anemic. The relationship between studied variables and anemia was evaluated by Poisson regression analysis. There was a 56.6% prevalence of anemia (95% CI: 46.6-54.6). Anemia was significantly correlated with low weight (Prevalence ratio - PR = 1.39; 95% CI: 1.18-1.64), young age (PR = 2.01; 95% CI: 1.57-2.56) and a diagnosis of acute lower respiratory disease (PR = 1.57; 95% CI: 1.27-1.96). CONCLUSION: The high prevalence of anemia suggests that it may contribute as a causal factor for hospitalization, especially because the period of hospitalization was short and the patient was likely to be anemic at the time of admission. This study stresses the importance of evaluating the overall nutritional status of patients, including their ingestion of microelements. This is especially important in children, because of their greater susceptibility to anemia. Measures directed at the prevention and control of anemia, including increased coverage of supplementation and fortification programs are strongly recommended.
Anemia; Prevalence; Nutritional status; Risk factors
ORIGINAL ARTICLE
Prevalence of anemia in under five-year-old children in a children's hospital in Recife, Brazil
Rosemary Ferreira dos SantosI; Eliane Siqueira Campos GonzalezII; Emídio Cavalcanti de AlbuquerqueII; Ilma Kruze Grande de ArrudaIII; Alcides da Silva DinizIII; José Natal FigueroaII; Ana Paula Campos PereiraII
IHospital Pediátrico Helena Moura, Recife, PE, Brazil
IIInstituto de Medicina Integral Professor Fernando Figueira - IMIP, Recife, PE, Brazil
IIINutrition Department, Centro de Ciências da Saúde, Universidade Federal de Pernambuco, Recife, PE, Brazil
Corresponding author Corresponding author: Ana Paula Campos Pereira Instituto de Medicina Integral Professor Fernando Figueira - IMIP Rua dos Coelhos, 300 - Boa Vista 50070-550 - Recife, PE, Brazil Phone: 55 81 2122-4702 apcamposp@hotmail.com
ABSTRACT
INTRODUCTION: Anemia is a nutritional problem of global importance. It is estimated that at least one-third of the population has been at one time anemic.
OBJECTIVE: To evaluate the prevalence of anemia and associated factors in patients of a children's hospital in Recife.
METHODS: A cross-sectional study was developed involving 595 male and female children aged from 6 to 59 months old, who were hospitalized in 2007.
RESULTS: Children with a hemoglobin concentration less than 11 g/dL were considered anemic. The relationship between studied variables and anemia was evaluated by Poisson regression analysis. There was a 56.6% prevalence of anemia (95% CI: 46.6-54.6). Anemia was significantly correlated with low weight (Prevalence ratio - PR = 1.39; 95% CI: 1.18-1.64), young age (PR = 2.01; 95% CI: 1.57-2.56) and a diagnosis of acute lower respiratory disease (PR = 1.57; 95% CI: 1.27-1.96).
CONCLUSION: The high prevalence of anemia suggests that it may contribute as a causal factor for hospitalization, especially because the period of hospitalization was short and the patient was likely to be anemic at the time of admission. This study stresses the importance of evaluating the overall nutritional status of patients, including their ingestion of microelements. This is especially important in children, because of their greater susceptibility to anemia. Measures directed at the prevention and control of anemia, including increased coverage of supplementation and fortification programs are strongly recommended.
Keywords: Anemia; Prevalence; Nutritional status; Risk factors
Introduction
Deficiency anemia is a significant public health problem that occurs worldwide in both developed and developing countries. In 1980, the World Health Organization (WHO) estimated that 700 million people worldwide suffered from anemia and more than two billion people worldwide have been affected by it. Approximately 50% of anemia cases are caused by iron deficiency.(1) In the Americans, the rate of anemia is especially high among children, with a prevalence of 50% in Mexico and between 45% to 70% in different regions of the Ecuador.(2,3) In Brazil, population-based studies conducted in several regions of the country have shown that the prevalence of anemia varies between 30% and 60%.(4,5) Batista & Migliolo found that approximately 45% of under 5-year-old children in Brazil were anemic.(6)
Most anemia cases develop gradually and progressively and are due to iron deficiency. In early childhood, bad feeding habits, especially during the weaning period, exacerbate the problem. Anemia frequently develops as breast milk is replaced by foods that are poor in iron and other nutrients, including vitamin B12 and folic acid.(7,8) Low oxygenation of brain tissues, a consequence of anemia, may lead to impaired cognitive function, growth and psychomotor development, especially in children.(9) Infants, under 5-year-old children and pregnant women have greater susceptibility to anemia because of their increased iron requirements due to rapid body growth and expansion of red blood cells.(10)
Anemia is associated with socioeconomic, biological, environmental and nutritional factors. In Brazil, population-based information is available on anemia in under 5-yearold children; however, data on this problem and associated factors in hospitalized children are scarce. Thus, this study aimed to estimate the prevalence of anemia and its relationship with biological and pathological factors in under 5-year-old children who were admitted to a public children's hospital in Recife.
Methods
This is a cross-sectional study conducted at the Hospital Pediátrico Helena Moura. This hospital is located in the city of Recife and treats medium complexity cases of children up to 15 years old. The hospital has 50 beds, of which 74.4% are occupied by residents of Recife. The other patients come from nearby municipalities (Olinda, Jaboatão, Camaragibe, Abreu and Lima). The charts of every child aged between 6 months and 5 years old who had been hospitalized between January and December 2007 and who had performed at least one blood test were analyzed. In total, 790 charts were analyzed and 595 patients were included in the study. Charts were excluded due to the absence of important data or when the patient was readmitted. Data pertaining to gender, age, weight, serum hemoglobin levels and the diagnosis that led to admission were collected.
Patients were categorized by age as follows: 6 - 11 months, 12 - 23 months, 24 - 35 months and > 36 months.
Routine procedures of the hospital were followed to measure hemoglobin with levels being determined using an ABX apparatus. Most patients only had one complete blood count (CBC), but for those with multiple CBC, only the first test was taken into account. The WHO criterion (hemoglobin < 11 g/dL) was used to diagnose anemia.(1) To categorize the degree of anemia, the following cut-off points were used: 10.0-10.9 g/dL - mild anemia; 7.0-9.9 g/dL - moderate anemia; < 7 g/dL - severe anemia.
A weight-for-age indicator was used to evaluate nutritional status. Weight was measured according to the routine procedures of the hospital. To analyze this variable, the z-score was used, with classification based on WHO standards: very underweight for age (z-score < -3); underweight for age (z-score > -3 and < -2); adequate weight (z-score > -2 and < +2) and overweight for age (z-score > +2).(11)
Pearson's chi-square test and linear regression were used to investigate the relationship between variables adopting an alpha value of 5% to reject the null hypothesis. The Marascuilo procedure was used to compare proportions between groups. Multivariate analysis was performed using Poisson regression for variables that had a significance level < 0.20 in the bivariate analysis. Statistical software was used to calculate nutritional status. Data were obtained using a secondary database, thus ensuring the privacy of the children included in the study. All children benefited from appropriate treatment for their condition during hospitalization. The study was approved by the Research Ethics Committee of the Instituto de Medicina Integral Professor Fernando Figueira (IMIP).
Results
Characterization of hospitalized children
This study included 595 children, whose characteristics are described in Table 1. The group was comprised of 54.3% boys and 45.7% girls. The predominant age group was between 12 and 24 months (31.3%). The majority of children were well-nourished (85.7%) and 22.5% were hospitalized for five or more days. Gastrointestinal (43.9%) and respiratory (21.3%) diseases were the most frequent reasons for hospitalization.
Prevalence of anemia and associated factors
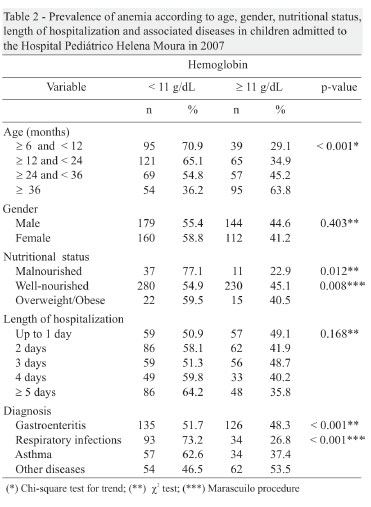
The results of the chi-square test for trend indicated that the proportion of anemic cases decreased with age, varying from 70.9% in children between 6 and 12 months to 36.2% in children 36 months and older (Table 2). These results were statistically significant (p-value = 0.001). There was no statistically significant difference in terms of gender (p-value = 0.403) with anemia affecting 55.4% of boys and 58.8% of girls. Anemia was significantly correlated with nutritional status (p-value = 0.012). When the Marascuilo procedure for multiple comparisons was applied, anemia was more prevalent among malnourished children than well-nourished children (p-value = 0.008). Comparisons between the remaining groups were not significant.
Anemia was more prevalent among children who were hospitalized for longer periods of time (64.2%) although this difference was not statistically significant (p-value = 0.168). In terms of diagnosis, the chi-square test indicated that there was a statistically significant association with the hemoglobin level (p-value < 0.001). The Marascuilo procedure indicated a significantly higher proportion of anemia cases in children with respiratory infections compared to those with gastroenteritis (p-value < 0.001) or other diseases (p-value < 0.001).
Multivariate analysis showed that children between 6 and 12 months of age had a 2-fold higher risk of having anemia (Prevalence ratio - PR = 1.9; p-value < 0.001). The risk of anemia increased by approximately 50% in children with respiratory infection (PR = 1.5; p-value < 0.001) and by almost 40% in malnourished children (PR = 1.4; p-value < 0.001). The length of hospitalization stay did not reach the level of statistical significance necessary for this variable to remain in the model. (Table 3)
Characterization of children in relation to hemoglobin levels
Figure 1 shows the distribution of hemoglobin levels. Overall, there was a 56.6% prevalence of anemia (95% CI: 46.6-54.6) and the average hemoglobin content was 10.5 g/dL ± 1.5 g/dL. Severe anemia was found in 1.8% (95% CI: 1.0-3.2) of children and the mildest form was found in 25.8% (95% CI: 22.4-29.4).
Discussion
Most studies on anemia are population-based; those conducted using a hospitalized population are scarce, which limits comparative analysis of results.
This study found a high prevalence of anemia, reflecting the magnitude of the disease among hospitalized children. Other studies in Recife have found similar results. Salzano reported the prevalence of anemia in 6 to 60-monthold children to be 55.1% in the Lessa de Andrade Health Center and 28.3% in Hospital Geral PAM, Areias.(12) In 2005, Leal & Osório reported a high prevalence (89.1%) in a state healthcare clinic in Recife.(13) Other reports analyzing state clinics in different regions of Brazil reported the prevalence in children to be 37.5% in Paraisópolis, São Paulo(14) and 55.1% in Belém do Pará.(15) For the state of Pernambuco, the III State Health and Nutrition Research found a prevalence of 33%.(16)
A high prevalence of anemia has also been reported in other Latin American countries. A population study conducted by Rivera, which focused on pre-school children in Cuba, reported a prevalence of 55.6%.(17) Sanabria reported a prevalence of 52% in under 5-year-old children in a referral hospital in Paraguay.(18) The prevalence of anemia found in this study, and in the abovementioned studies, was higher in specific population groups, indicating that the condition is influenced by socioeconomic status.
The prevalence of the problem in under 24-month-old children is likely to be a combined result of the increased iron requirements due to rapid growth, early weaning, low availability of foods rich in iron and dietary monotony. These factors are prevalent in this age group. Furthermore, unfavorable socioeconomic conditions impose living conditions that make children more vulnerable to diarrhea, respiratory infections and intestinal parasites, and may markedly compromise intake, absorption and biological utilization of iron. Neves,(15) studying 6 to 24-month-old children in a State Health-School Service in Belém, Pará, found a prevalence of anemia of 55.1%.
The influence of gender on anemia shows conflicting results. This and other studies found no association between anemia and gender,(19,20) whereas other authors reported that anemia is more common in boys.(8,21) An association with boys may be due to the faster growth of pre-school boys compared to girls, which results in a high iron demand that cannot be met by diet alone. However, further studies are necessary to better understand this factor.
The population studied follows the current trend of reduced malnutrition (8.2%) and increased incidence of obesity (6.2%). The increase in obesity in the population is a result of a nutritional and epidemiological transition experienced by different countries, including Brazil.(22) Although anemia was found predominantly in underweight children, it was also found in overweight children. A lack of vitamins and minerals is commonly observed in both of these conditions. The diet of obese or overweight children is often characterized by excessive calories and insufficient intake of vitamins and minerals. In children with some degree of malnutrition, in addition to the mineral deficiency, there is also a calorie and protein deficiency. Osório et al. also found a higher prevalence of anemia in malnourished children aged between 6 and 59 months in Pernambuco.(5) However, other studies, such as that of Neumann et al., which focused on under three-year-old children in southern Brazil, found no association.(4)
Anemia was, to a certain extent, associated with the reason for hospitalization. Anemia was most common in children suffering from respiratory tract diseases, followed by gastrointestinal diseases, those with other types of infection and finally non-infectious diseases. Respiratory tract diseases possibly require greater utilization of hemoglobin both due to the infectious process and increased respiratory effort, whereas gastrointestinal diseases lead to blood loss in feces and vomit or by degradation by parasites. Lima et al. reported a higher prevalence of anemia in infants with infectious diarrhea.(23) The diseases occurring in the study population raised questions about functional iron deficiency, which occurs when sufficient iron is not released to meet the normal hemoglobinization of red blood cells, either because of an absence of iron stores (iron-deficiency anemia) or by blocking iron homeostasis (anemia of inflammation). Anemia of inflammation, which is common in cases of inflammation and/ or infection, is an immune-mediated process in which cytokines and cells of the reticuloendothelial system induce changes that interfere in different erythropoiesis pathways leading to anemia.(24) Therefore, patients with anemia of inflammation may present associated iron deficiency, just as patients with iron deficiency anemia may develop anemia of inflammation.
The relationship between anemia and infection remains controversial. Anemia is an immunosuppressive factor, as mild iron deficiency protects against infection, because hypoferremia reduces the amount of iron available for use by pathogens.(25) In contrast, humoral immunity is not affected by iron deficiency, and the significance of hypoferremia in the growth of microorganisms is doubtful.(26) However, it is generally accepted that excess or deficiency of iron result in changes in immune response.(27)
The role of anemia on the average time of hospitalization is difficult to interpret, given that the length of stay may be related to other factors such as the severity of the clinical condition, different medical procedures and care, and random errors.(28) In this study, although the length of the hospital stay was not significantly associated with anemia, it is possible that anemia resulting from nutritional and immunological conditions aggravated the primary disease, thereby prolonging hospitalization.
The high prevalence of anemia reported here suggests that this condition may be an associated causal factor, especially as the length of hospitalization was generally short, and the patient was probably anemic at the time of admission. Our results emphasize the importance of evaluating the overall nutritional status of patients, especially children, because of their greater susceptibility. They also suggest that greater preventive nutritional education during consultations and/or hospitalizations and more attention from professionals at the primary care level, are needed to prevent nutritional deficiencies. This study makes us think about the necessity of expanding coverage of supplementation programs in order to help a larger number of at-risk individuals.
Submitted: 7/6/2010
Accepted: 11/10/2010
Conflict-of-interest disclosure: The authors declare no competing financial interest
References
- 1 World Health Organization. Iron deficiency anemia assessment, prevention and control. A guide for programme managers. Geneva; WHO; 2001.
- 2. Villapando S, Shamah LT, Ramirez-Silva CI, Nejia-Rodrigues F, Rivera JA. Prevalence anemia in children to 12 years of age. Results from a nation wide probabilistic survey in Mexico. Salud Publica Mex. 2003;45 Suppl 4:490-8.
- 3. Freire WB, Dirren H, Barclay D. Iron deficiency anemia in Ecuador. In: Hercberg S, Galan P, Dupin H. Recent knowledge on iron and folate deficiencies in the world. Paris: Collogue INSEAM;1990.p. 47-54.
- 4. Neuman NA, Tanaka OY, Szarfarc SC, Guimarães PR, Victora CG. Prevalência e fatores de risco para anemia no Sul do Brasil. Rev Saúde Pública.2000;34(1):56-63.
- 5. Osório MM, Lira PIC, Batista-Filho M, Ashworth A. Prevalence of anemia in children 6-59 months old in the state of Pernambuco, Brazil. Rev Panam Salud Publica. 2001;10(2):101-7.
- 6. Batista Filho M, Migliolo TC. Alimentação e nutrição no nordeste do Brasil. Recife: Instituto Materno Infantil Professor Fernando Figueira (IMIP); 2006.
- 7. Rolo S, Morgado M. Anemia: terapêutica farmacológica. Rev de la Ofil. 2006;(16):34-40.
- 8. Torres MA, Sato K, Queiroz SS. [Anemia in children under 2 years in basic health care units in the State of São Paulo, Brazil]. Rev Saúde Pública 1994;28(4):290-4. Portuguese.
- 9. Walter T, de Andraca I, Chadud P, Perales CG. Iron deficiency anemia: adverse effects on infant psychomotor development. Pediatrics.1989;84(1):7-17.
- 10. Silva DG, Franceschini SC, Priore SE, Ribeiro SM, Szarfarc SC, Souza SB, et al. Anemia ferropriva em crianças de 6 a 12 meses atendidas na rede pública de saúde do município de Viçosa, Minas Gerais. Rev Nutr. 2002;15(3):301-8.
- 11. World Health Organization. WHO child growth standards: length/height-for-age, weight-for-length, weight-for-height: and body mass index-for-age. Methods and development. WHO (nonserial publication). Geneva, Switzerland: WHO; 2006.
- 12. Salzano CA, Torres MA, Batista Filho M, Romani SA. [Anemia in children at 2 health centers in Recife, PE (Brazil)]. Rev Saúde Pública. 1985;19(6):499-507. Portuguese.
- 13. Leal LP, Osório MM. [Validity and reproducibility of the clinical signs for the Diagnosis of anemia in children]. Cad Saúde Pública. 2005;21(2):565-72. Portuguese.
- 14. Torres MA, Braga JA, Taddei JA, Nóbrega FJ. [Anemia in lowincome exclusively breastfed infants]. J Pediatr (Rio J). 2006;82 (4):284-7. Portuguese.
- 15. Neves MB, Silva EM, Moraes MB. [Prevalence and factors associated with iron deficiency in infants treated at a primary carecenter in Belém, Pará, Brazil]. Cad Saúde Pública. 2005;21 (6):1911-8. Portuguese.
- 16. III Pesquisa Estadual de Saúde e Nutrição - Pernambuco, 2006 DN/UFPE IIMIPSES/PE. [cited 2011 Apr 5]. Available from: http://pesnpe2006.blogspot.com/2008/09/apresentao-dapesquisa.html
- 17. Rivera JA, Amor JS. Conclusions from the Mexican National Nutrition Survey 1999: translating results into nutrition policy. Salut Pública de Méx. 2003;(4):565-75.
- 18. Sanabria MC, Dietz E, Varela CA. Evaluación nutricional de niños hospitalizados en un servicio de pediatria de referencia. Pediatr. (Asunción);27(1):16-23.
- 19. Rocha DS, Lamounier JÁ, Capanema FD, Franceschini SC, Norton RC, Costa AB, et al. Estado nutricional e prevalência de anemia em crianças que frequentam creches em Belo Horizonte, Minas Gerais. Rev Paul Pediatr. 2008;26(1):6-13.
- 20. Silva LS, Giugliani ER, Aerts DR. [Prevalence and risk factors for anemia among children in Brazil]. Rev Saúde Pública. 2001; 35(1):66-73. Portuguese.
- 21. Oliveira RS, Diniz AS, Benigna MJ, Silva SM, Lola MM, Gonçalves MC, et al. Magnitude, distribuição espacial e tendência da anemia em pré-escolares da Paraíba. Rev Saúde Pública. 2002; 36(1):26-32.
- 22. Batista Filho M, Rissin A. Nutritional transition in Brazil: geographic and temporal trends. Cad Saúde Pública. 2003;19 Suppl 1:S181-91. Portuguese.
- 23. Lima AC, Lima MC, Guerra MQ, Romani SA, Eickmann SH, Lira PI. Impact of weekly treatment with ferrous sulfate on hemoglobin level, morbid and nutritional status of anemic infants. J Pediatr (Rio J). 2006;(82):452-7. Comment in: J Pediatr (Rio J). 2007; 83(1):95; author reply 95-6.
- 24. Figueiredo MS. Impacto da inflamação na regulação do ferro e deficiência funcional de ferro. Rev Bras Hematol Hemoter. 2010; 32 Supl 2:18-21.
- 25. Jansson LT, Kling S, Dallman PR. Anemia in children with acute infections seen in a primary care pediatric outpatient clinic. Pediatr Infect Dis. 1986;5(4):424-7.
- 26. Krantman HL, Young SR, Ank BJ, ODonnell CM, Rachelefsky GS, Stiehm ER. Immune function in pure iron deficiency. Am J Dis Child. 1982;136(9):840-4.
- 27. Umbelino DC, Rossi EA. Deficiência de ferro: conseqüências biológicas e propostas de prevenção. Rev Ciênc Farm Básica Apl. 2006;27(2):103-12.
- 28. Travassos C, Noronha JC. Martins M. Morbidade hospitalar como indicador de qualidade: uma revisão. Ciênc Saúde Coletiva. 1999;4(2):367-81.
Publication Dates
-
Publication in this collection
13 June 2011 -
Date of issue
2011
History
-
Received
06 July 2010 -
Accepted
10 Nov 2010